LORVIQUA can offer >7 years of PFS, the longest PFS ever reported in advanced lung cancer 1**
3% of patients on crizotinib (hazard ratio 0.19 [95% CI: 0.13–0.26])1
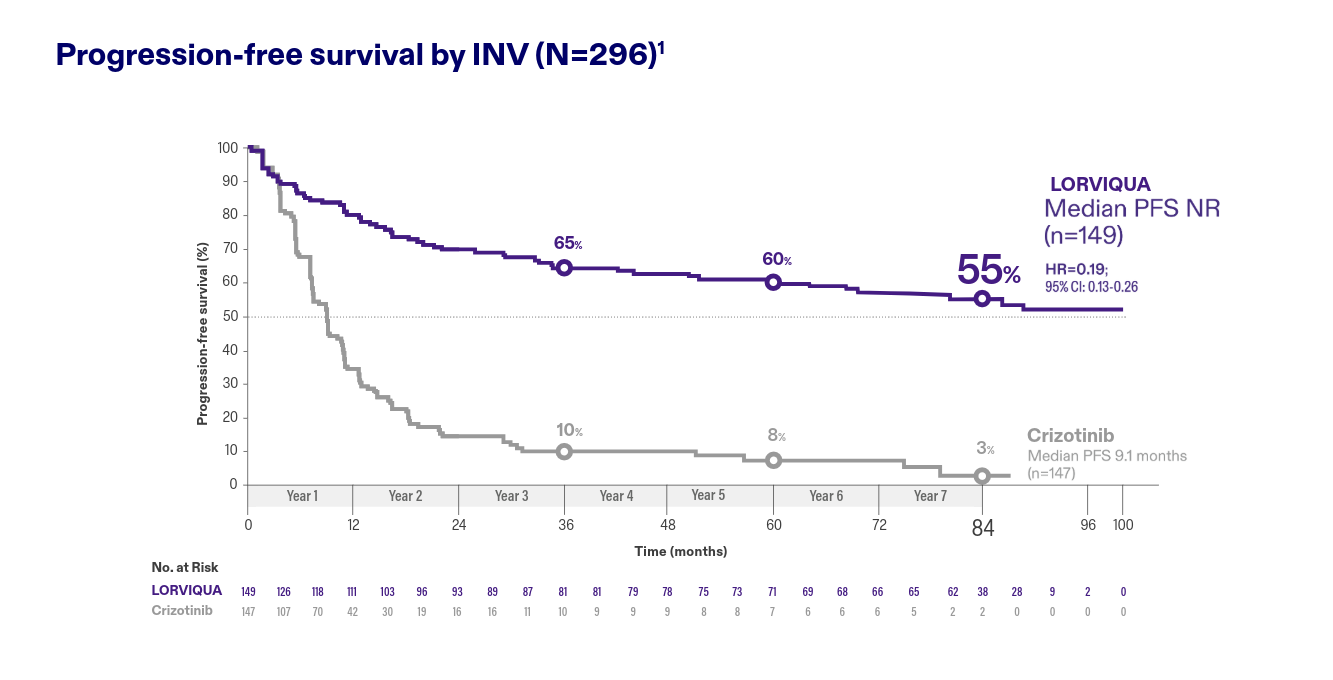
Adapted from Shaw AT, et al. Ann Oncol. 20261
Data cutoff 31 October 2025.1
Patients who were event free at 2 years had a 79% probability of being alive and progression free at 7 years †‡§
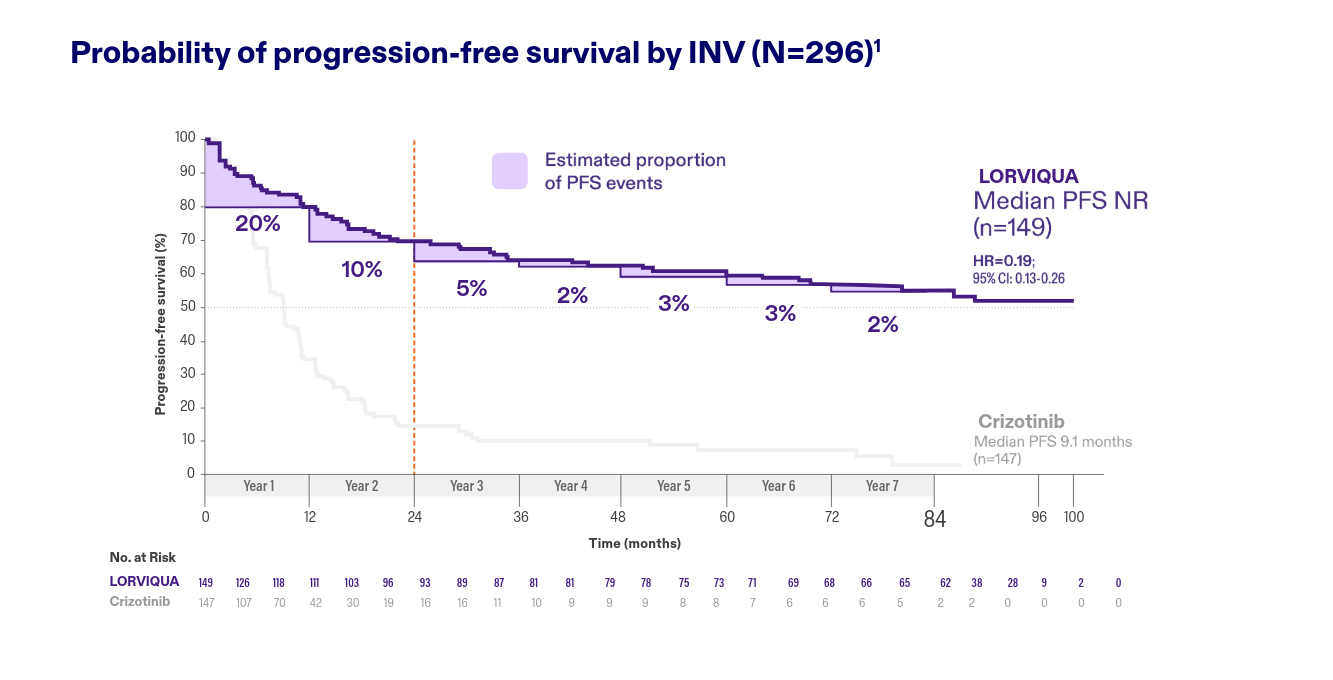
Adapted from Shaw AT, et al. Ann Oncol. 20261
Data cutoff 31 October 2025.1
LORVIQUA can offer durable control and prevention of brain metastases at 7 years 1†‡
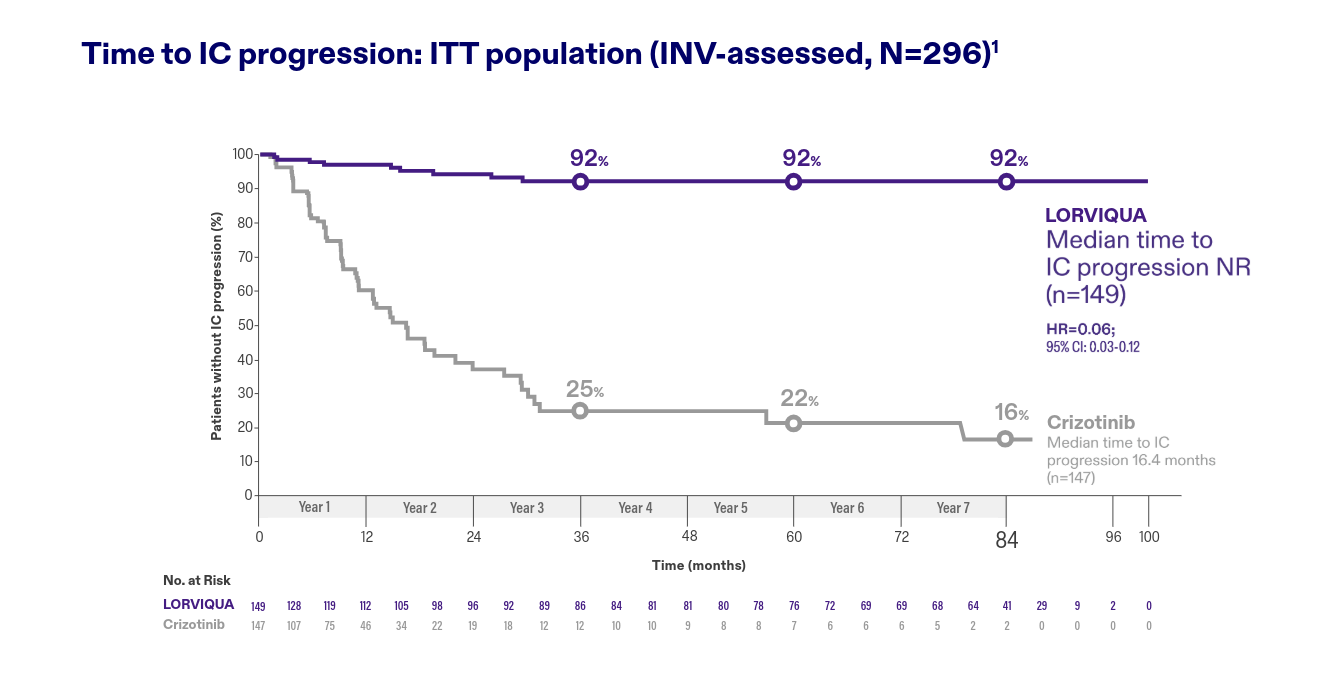
Adapted from Shaw AT, et al. Ann Oncol. 20261
Data cutoff 31 October 2025.1
Key safety summary
The safety profile for LORVIQUA in the 7-year follow-up
analysis was consistent with that in the primary analysis.
No new safety signals emerged1
- No new treatment discontinuations due to TRARs after the first 26 months1
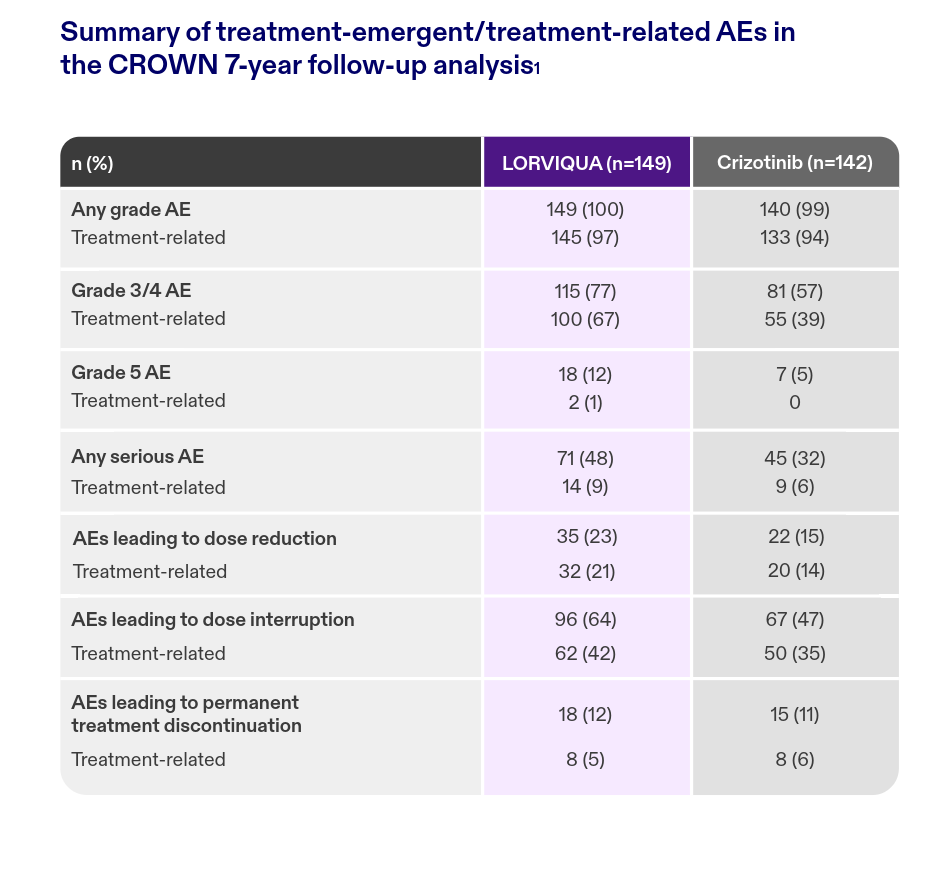
Adapted from Shaw AT, et al. Ann Oncol. 20261
Therapy management considerations
Most ARs occurred within the first 6 months and can be managed with appropriate mitigation strategies5
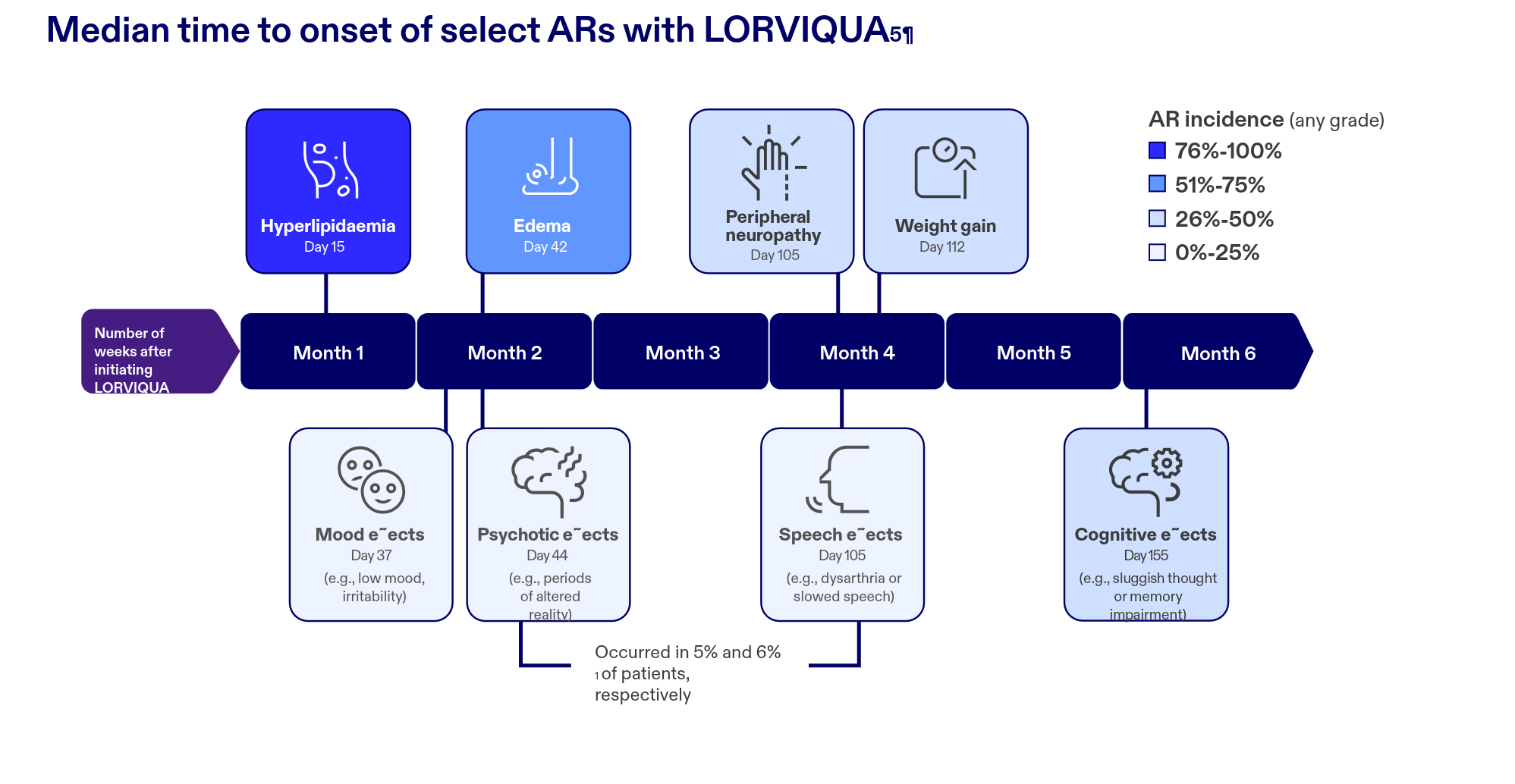
Adapted from Liu G, et al. Lung Cancer. 2024
CNS effects
Weight gain
- Lifestyle changes may include a low-calorie, healthy diet and regular exercise5
Hyperlipidaemia
- Choose either rosuvastatin or pravastatin5
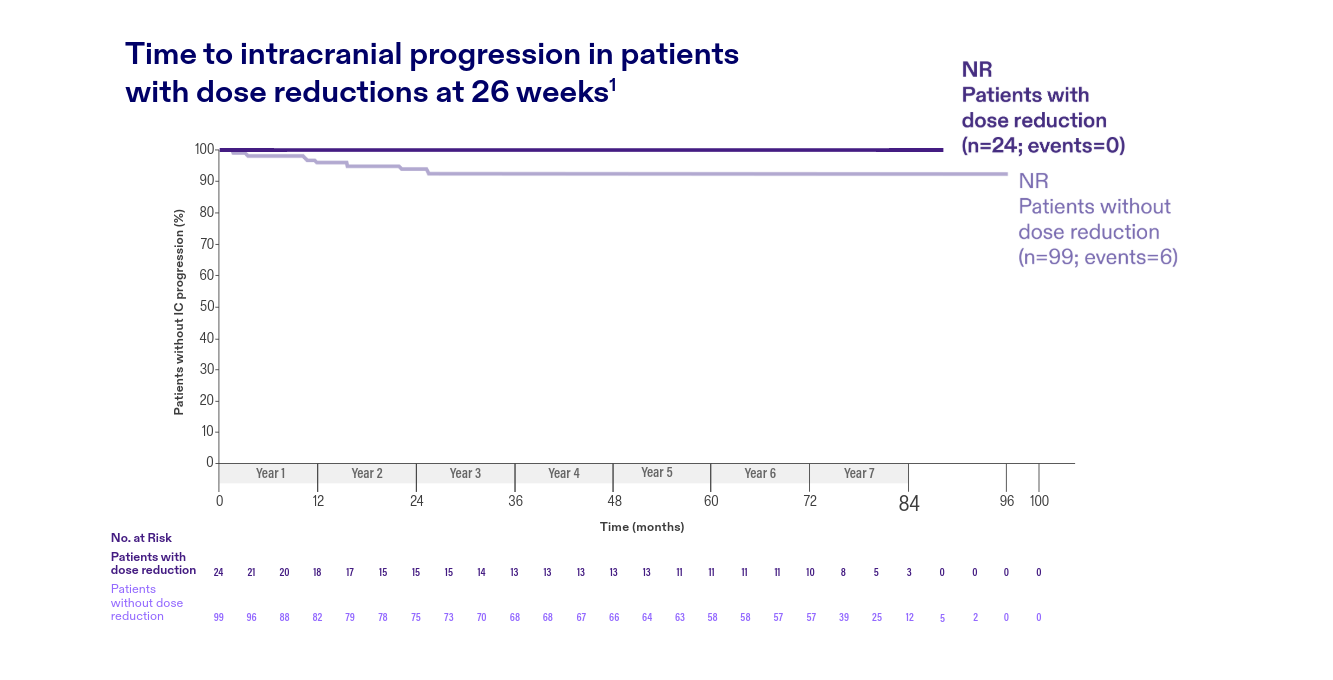
Dose modifications
Dose reductions did not compromise systemic or intracranial efficacy1‡‡

Adapted from Shaw AT, et al. Ann Oncol. 20261
Adapted from Shaw AT, et al. Ann Oncol. 20261
†The primary endpoint of PFS was met in the CROWN trial BICR-assessed primary analysis
(median follow-up for PFS: 18.3 months for patients receiving LORVIQUA and 14.8 months for
patients receiving crizotinib); median PFS was not estimable for the LORVIQUA arm. An
unplanned INV-assessed follow-up analysis was performed at a median follow-up for PFS of
approximately 83 months for patients on LORVIQUA (77.2 months for patients on crizotinib) to
confirm the effect of LORVIQUA relative to crizotinib with longer follow-up. All tumour-related
endpoints reported in the 7-year analysis are INV-assessed.1,3
‡LIMITATIONS: The results of this unplanned, INV-assessed analysis are descriptive. No formal
hypothesis testing was performed given that the PFS endpoint was previously met in the
CROWN trial primary analysis; results are presented descriptively.1
§Event equals progression or death.1
¶The values listed here represent median time to first occurrence for each AR. There is a
distribution in which some may occur earlier or later than these median values.4
**CNS effects included cognitive, mood, speech and psychotic effects.1
‡‡Based on data from 84-month follow-up of 149 patients who received LORVIQUA 100 mg once
daily in the Phase 3 CROWN trial.1
LORVIQUA® is indicated for the treatment of adult patients with metastatic non-small cell lung cancer (NSCLC) whose tumors are anaplastic lymphoma kinase (ALK)-positive4.
Adverse Reactions: The most common adverse reactions (occurring in ≥20% of patients) include edema, peripheral neuropathy, cognitive effects, dyspnea, fatigue, weight gain, arthralgia, mood effects, and diarrhea. The most common laboratory abnormalities (occurring in ≥20% of patients) include hypercholesterolemia, hypertriglyceridemia, anemia, hyperglycemia, increased AST, hypoalbuminemia, increased ALT, increased lipase, and increased alkaline phosphatase. Adverse reactions should be managed according to severity-based dose modification recommendations.
For further information including: safety information, indication, side effects, contraindications, special warnings and precautions for use, please refer to the latest approved Israel prescribing information.
Abbreviations:
1L=first-line; AE=adverse event; ALK+=anaplastic lymphoma kinase-positive; aNSCLC=advanced non-small cell lung cancer;
AR=adverse reaction; BICR=Blinded Independent Central Review; CI=confidence interval; CNS=central nervous system;
HR=hazard ratio; IC=intracranial; INV=investigator; ITT=intention-to-treat; NR=not reached; PFS=progression-free survival;
SmPC, Summary of Product Characteristics; TKI=tyrosine kinase inhibitor; TRAR=treatment-related adverse reaction.
References:
1. Shaw AT, et al. Ann Oncol. 2026; doi: https://doi.org/10.1016/j.annonc.2026.05.692;
2. Solomon BJ, et al. J Clin Oncol. 2024;42(29):3400–3409;
3. Shaw AT, etal. N Engl J Med. 2020;383(21):2018–2029;
4. The latest approved LORVIQUA Israeli prescribing information;
5. Liu G, et al.Lung Cancer. 2024;191:107535;
6. Liu G, et al. Oncologist. 2025;30(10)oyaf287;
7. Liu G, et al. Presented at ASCO 2025,30 May–3 June, Chicago, USA. Abstract 8590.